
Blepharitis
Diagnosis and treatment of eyelid margin inflammation — anterior and posterior blepharitis, meibomian gland dysfunction, and Demodex infestations.
What is Blepharitis
Blepharitis is a chronic inflammation of the eyelid margins. It is one of the most common eyelid conditions seen by eye physicians and oculoplastic surgeons, affecting patients of all ages. Although rarely vision-threatening in its early stages, untreated blepharitis causes progressive discomfort, contributes to dry eye disease, and can lead to corneal damage and eyelid structural changes over time.
Blepharitis and Dry Eye Disease are closely linked — each worsens the other. Treating meibomian gland dysfunction (posterior blepharitis) is central to managing both. Ocular rosacea is a related condition covered on the Rosacea page.
Types of Blepharitis
Blepharitis is classified by anatomical location and underlying cause:
Anterior Blepharitis
Affects the front of the eyelid margin where the eyelashes are attached.
- Staphylococcal — bacterial colonization of lash follicles; produces cylindrical collarettes (scurf) at lash bases
- Seborrheic — greasy, flaky scales; associated with seborrheic dermatitis of the scalp and face
- Demodex — infestation of lash follicles by Demodex folliculorum mites; produces characteristic cylindrical sleeves around lash roots
Posterior Blepharitis
Affects the meibomian gland orifices at the inner eyelid margin (lid wiper).
- Meibomian Gland Dysfunction (MGD) — obstruction of meibomian gland ducts leading to altered lipid secretion; the most common cause of evaporative dry eye
- Rosacea-associated — facial rosacea commonly involves meibomian glands; see Rosacea page
Symptoms
- Burning, stinging, or itching of the eyelids — typically worse in the morning
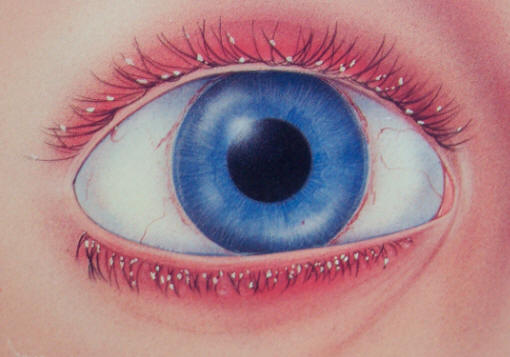
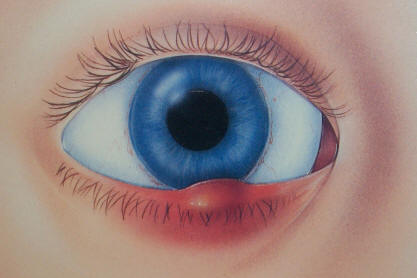
- Red, irritated eyelid margins with visible crusting or scaling at the lash bases
- Eyelids stuck together on waking
- Fluctuating blurred vision from unstable tear film (blinks transiently clear vision)
- Gritty or foreign body sensation
- Photosensitivity
- Recurrent chalazia (blocked meibomian gland cysts)
- Lash loss (madarosis) in severe, long-standing cases
Clinical Findings
Slit lamp examination reveals distinct features depending on type:
- Anterior (staph): Collarettes — hard, brittle scales adherent to lashes near follicles. Lash thinning or misdirection (trichiasis). Marginal corneal infiltrates in severe cases.
- Anterior (seborrheic): Soft, greasy flakes on lashes without underlying ulceration. Less follicular involvement than staphylococcal.
- Demodex: Cylindrical sleeves — translucent sheaths surrounding the base of lashes. High-magnification or epilated lash examination shows mites.
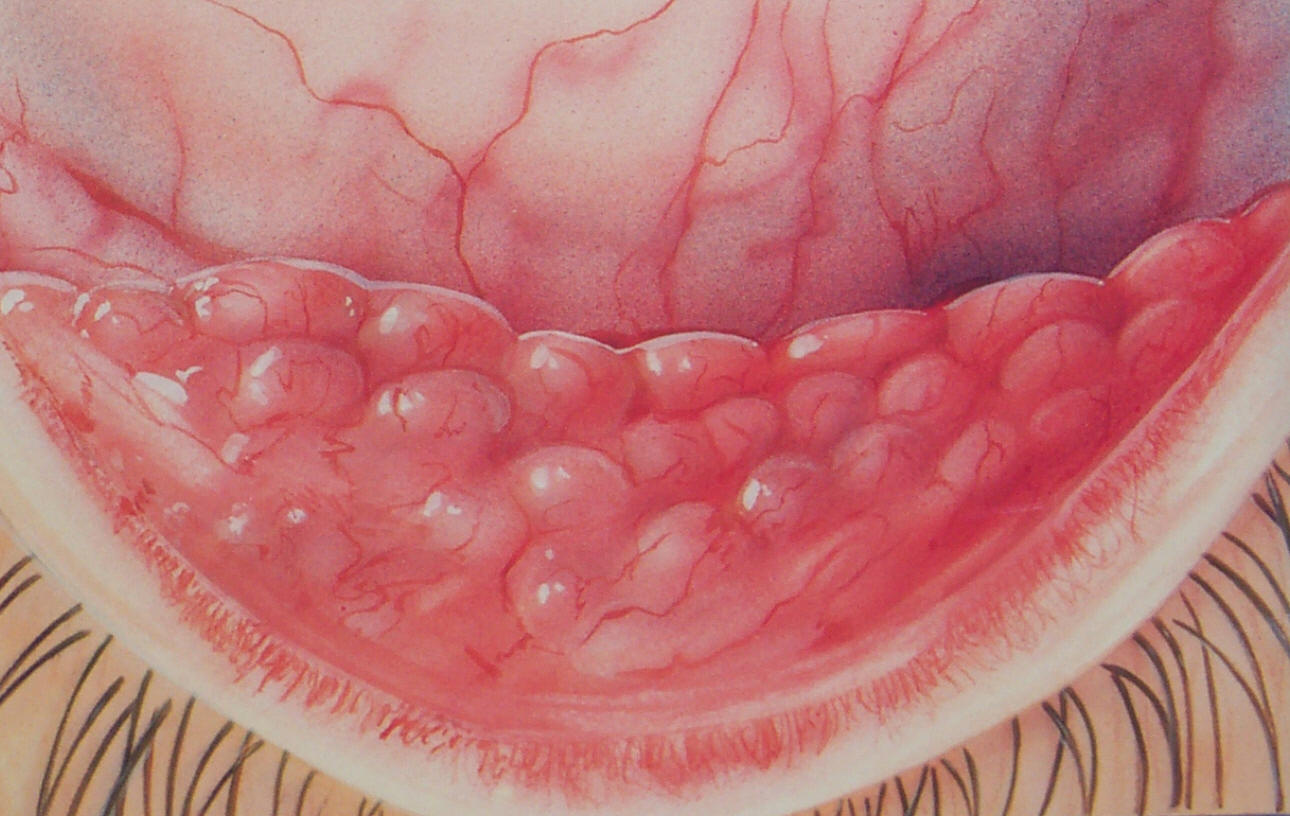
- Posterior (MGD): Plugged or capped meibomian orifices. Inspissated (thickened, toothpaste-like) or absent meibomian secretion. Vascular engorgement and notching of the lid margin. Tear break-up time typically shortened.
Meibography (infrared imaging) reveals gland dropout in chronic MGD — evidence of permanent glandular damage in advanced disease.
Treatment
Blepharitis is a chronic condition requiring long-term management. No single treatment is curative, but consistent hygiene and appropriate therapy significantly reduce inflammation and symptoms.
Eyelid Hygiene
The cornerstone of blepharitis management. Removes debris, unclogs meibomian orifices, and reduces bacterial load:
- Warm compresses: Applied to closed lids for 5–10 minutes to melt inspissated meibum. A warm, moist cloth or a dedicated eyelid warming mask (e.g., Bruder mask) is used. Essential for posterior blepharitis and MGD.
- Lid massage: After warming, gentle rolling pressure along the lid margin expresses liquefied meibum from gland orifices.
- Lid scrubs: Dilute baby shampoo or commercial eyelid wipes (OCuSOFT, Systane, Cliradex) clean lash debris and reduce bacterial colonization. Applied with a cotton tip or pad to the eyelid margin in a scrubbing motion.
Antibiotic Therapy
- Topical antibiotics: Azithromycin ophthalmic solution or erythromycin ointment applied to the eyelid margin reduces bacterial colonization and inflammation. Azithromycin (AzaSite) has anti-inflammatory properties in addition to its antibiotic effect.
- Oral doxycycline: Low-dose doxycycline (50–100 mg daily) has both antibiotic and significant anti-inflammatory effects on meibomian gland function. First-line systemic therapy for moderate-to-severe posterior blepharitis and MGD. Typical course: 1–3 months, sometimes longer in rosacea-associated blepharitis. Side effects: photosensitivity, GI upset.
- Oral tetracycline, minocycline: Alternatives to doxycycline with similar mechanism.
Demodex-Specific Treatment
For Demodex blepharitis, eyelid tea tree oil (4-terpineol) scrubs or weekly in-office treatments are effective. XDEMVY (lotilaner ophthalmic solution 0.25%) — FDA-approved specifically for Demodex blepharitis — is applied twice daily for 6 weeks and has demonstrated significant reduction in mite counts and collarettes in clinical trials.
In-Office Procedures
- BlephEx: Mechanical debridement of the eyelid margin using a rotating micro-sponge device. Removes biofilm, collarettes, and debris; unclogs meibomian orifices.
- Intense Pulsed Light (IPL): Treats posterior blepharitis by applying pulsed light to the periocular skin, heating meibomian glands, reducing Demodex populations, and reducing telangiectasias. Multiple sessions (3–4) spaced 3–4 weeks apart.
- Thermal pulsation (LipiFlow): Applies simultaneous heat to the inner eyelid surface and pulsatile pressure to express inspissated meibomian gland content. A single 12-minute treatment per eye.
- Manual expression: Meibomian gland expression in clinic using paddles or forceps after lid warming — directly clears obstructed glands.
Complications of Untreated Blepharitis
- Chalazion: Chronic blockage of meibomian glands progresses to a lipogranulomatous cyst (chalazion). Recurrent chalazia are often a sign of underlying posterior blepharitis or MGD.
- Meibomian gland dropout: Progressive glandular atrophy visible on meibography — permanent loss of gland tissue leading to irreversible dry eye.
- Marginal keratitis: Peripheral corneal infiltrates from immune reaction to staphylococcal antigens — may require topical steroids.
- Corneal neovascularization and pannus: In severe, longstanding cases.
- Trichiasis and madarosis: Misdirected or lost lashes from chronic follicular inflammation.
- Worsening dry eye: Meibomian lipid deficiency accelerates tear evaporation and perpetuates the blepharitis-dry eye cycle.
Frequently Asked Questions
- What is blepharitis?
- Blepharitis is chronic inflammation of the eyelid margins. Anterior blepharitis affects the eyelid skin and lash follicles (often related to Staphylococcus bacteria or Demodex mites). Posterior blepharitis (meibomian gland dysfunction, or MGD) affects the oil-secreting glands inside the eyelid and is the leading cause of evaporative dry eye.
- How is blepharitis treated?
- Treatment depends on type. All forms benefit from warm compresses and eyelid margin hygiene. Anterior blepharitis may require topical antibiotics or tea tree oil scrubs (for Demodex). MGD/posterior blepharitis is treated with oral omega-3 fatty acids, doxycycline, in-office thermal treatments (LipiFlow, iLux), or intense pulsed light (IPL) therapy.
- Does blepharitis ever go away completely?
- Blepharitis is typically a chronic condition that requires ongoing management rather than a one-time cure. With consistent lid hygiene and appropriate treatment, most patients achieve good symptom control. Flares can occur with stress, illness, or lapses in hygiene.
- When should I see an oculoplastic specialist for blepharitis?
- You should consider consulting an oculoplastic specialist if you have chronic blepharitis that hasn't improved with standard treatments like eyelid hygiene and topical medications, or if you experience severe symptoms affecting your quality of life. Additionally, if you have complications such as recurrent styes, chalazia, or eyelid margin scarring, a specialist can provide advanced diagnostic techniques and targeted treatments. Specialists can also identify underlying conditions like Demodex infestations or meibomian gland dysfunction that may require specialized management.
- What can I expect during my blepharitis consultation?
- During your consultation, the specialist will perform a thorough examination of your eyelids using magnification and specialized lighting to assess the severity of inflammation and identify the type of blepharitis you have. They may use imaging technology such as meibography to evaluate meibomian gland structure and function. You'll discuss your symptoms, current treatment regimen, and medical history to develop a personalized treatment plan that may include in-office procedures, medications, or lifestyle modifications.
- What are the potential risks and complications of blepharitis treatments?
- Most conservative blepharitis treatments like lid hygiene and topical medications have minimal risks, though some patients may experience mild irritation or allergic reactions to eye drops or ointments. In-office procedures such as lid margin debridement or meibomian gland expression are generally safe but carry rare risks of temporary discomfort or minor bleeding. More advanced treatments like intense pulsed light therapy or thermal procedures have excellent safety profiles when performed by experienced specialists, though some patients may experience transient redness or mild irritation.
- What is involved in long-term management of blepharitis?
- Long-term blepharitis management typically requires ongoing eyelid hygiene practices, including daily warm compresses and gentle cleansing of the eyelid margins to prevent recurrence. Many patients benefit from periodic in-office treatments or maintenance procedures to manage symptoms and prevent complications. Your specialist will recommend a maintenance schedule and may adjust your treatment plan based on your response, ensuring you maintain comfort and eye health over time.
Find a Specialist
Connect with a board-certified oculoplastic surgeon who specializes in blepharitis.
Search the Directory →