Periocular Rejuvenation
A comprehensive approach to restoring a rested, youthful periocular appearance through coordinated surgical and non-surgical treatments.
Overview
The eyes are the most expressive feature of the human face and often the first area to show signs of aging. Subtle changes in the skin, fat compartments, muscles, and bony architecture around the eyes can make a person appear tired, sad, angry, or older than they feel. Periocular rejuvenation is the coordinated practice of restoring a rested, refreshed, and natural appearance to the upper face through a thoughtful combination of surgical and non-surgical techniques.
Unlike a single procedure approach, true periocular rejuvenation considers the entire upper third of the face as an interconnected aesthetic unit. The brow position influences upper eyelid appearance. Tear trough hollowness affects how lower eyelid bags look. Skin quality, dynamic wrinkles, and volume loss all interact. A patient who receives only a lower blepharoplasty when the real problem is midface descent will be disappointed; a patient who gets filler in the tear trough when they truly need surgical fat repositioning may end up looking worse, not better.
This page serves as a comprehensive guide to the full spectrum of periocular rejuvenation. It explains how the area ages, reviews the surgical and non-surgical options available, and discusses how an oculoplastic surgeon — uniquely trained in both functional and aesthetic eyelid surgery — approaches treatment planning.

New to oculoplastic care? Start with What Is an Oculoplastic Surgeon to understand the specialized training behind eyelid and periocular aesthetics.
Anatomy of Aging
To understand why periocular rejuvenation requires a multi-layered approach, it helps to know what actually changes with time. Aging around the eyes is not a single process — it is the simultaneous deterioration of several anatomic layers.
Skin and Surface Changes
The eyelid skin is the thinnest on the human body, often less than one millimeter thick. With time, ultraviolet exposure, and repeated muscle contraction, this skin loses elastin and collagen. Fine etched lines (“crow’s feet”) form at the lateral canthus. Pigment irregularities, broken capillaries, and dull texture accumulate. Crepey skin develops on the upper and lower lids.
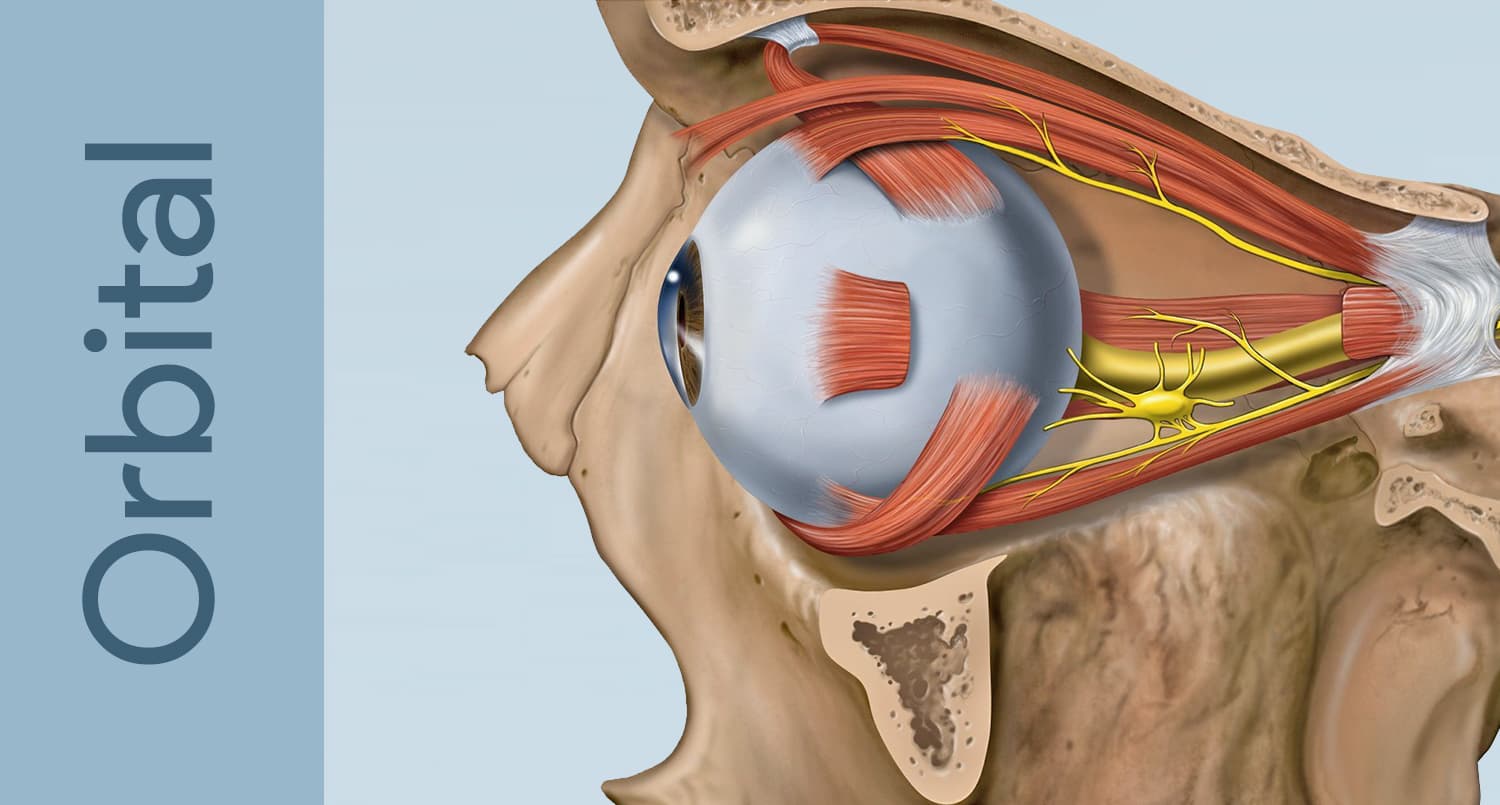
Muscle and Dynamic Changes
The orbicularis oculi muscle encircles the eye and is responsible for blinking and squinting. Decades of contraction produce dynamic wrinkles — crow’s feet laterally, fine lines below the lower lid margin, and bunching at the lateral orbital rim. The frontalis and corrugator muscles of the forehead contribute to horizontal forehead lines and vertical “11s” between the brows.
Fat Compartment Changes
Orbital fat behaves predictably with age. In the upper lid, the medial fat pad often becomes prominent, creating fullness near the nose. In the lower lid, the medial, central, and lateral fat pads herniate forward as the orbital septum weakens, producing visible “bags.” At the same time, fat in the brow, temple, and midface deflates, creating hollowness above and below the eye. This combination of fat herniation in some areas and fat loss in others creates the classic tired appearance.
Bone and Structural Changes
The orbital rim itself remodels over decades. The infraorbital rim recedes, deepening the tear trough. The lateral brow loses bony support. The maxilla rotates posteriorly. These changes mean that even with perfect skin and ideal fat distribution, the underlying scaffold of the face has shifted.
Brow and Midface Descent
The lateral brow descends with age, crowding the upper eyelid and creating a perception of upper lid heaviness that may actually be a brow problem. The midface descends, exposing the bony orbital rim and worsening tear trough deformity. Upper facial aging and midface aging are inseparable from eyelid appearance.
Important: Treating a single layer of aging in isolation often produces unnatural results. A blepharoplasty performed without addressing brow descent can lower the brow further; filler placed without considering volume loss elsewhere can look lumpy or puffy.
Surgical Options
Surgical periocular rejuvenation addresses problems that volume and energy-based treatments cannot fix — namely, excess skin, herniated fat, and significant structural descent. Surgery offers the most durable and dramatic improvements, but requires appropriate patient selection.
Upper Blepharoplasty
Upper blepharoplasty removes redundant upper eyelid skin and, when appropriate, a small strip of orbicularis muscle and prolapsed medial fat. It is one of the most reliably gratifying cosmetic procedures available. Patients describe their eyes feeling lighter and more open. The procedure is performed through a hidden incision in the natural lid crease and typically takes under an hour per side.
Lower Blepharoplasty
Lower blepharoplasty addresses under-eye bags and excess lower lid skin. Modern technique emphasizes fat repositioning rather than aggressive fat removal — the herniated fat is mobilized over the orbital rim to fill the tear trough, simultaneously fixing the bag and the hollow. The transconjunctival approach (incision inside the lid) leaves no visible scar. Skin laxity, if present, can be addressed with a small subciliary skin pinch or laser resurfacing.
Brow Lift
A brow lift restores brow position when descent contributes to upper lid heaviness. Modern endoscopic and direct techniques produce subtle, natural elevation — not the “surprised” look of older surgeries. For some patients, a small brow lift combined with conservative upper blepharoplasty gives a far better result than aggressive skin removal alone.
Midface Lift
A midface lift repositions the descended cheek pad, recreating support beneath the lower eyelid and softening the lid-cheek junction. It is particularly valuable for patients with prominent festoons or malar mounds.
Fat Grafting
Autologous fat grafting uses the patient’s own fat — harvested by gentle liposuction from the abdomen or thigh — to restore volume to the temple, brow, tear trough, and cheek. Because the result uses living tissue, it can be permanent and feels completely natural.
Non-Surgical Options
Non-surgical periocular treatments have transformed aesthetic practice over the past two decades. They are ideal for younger patients, for maintenance between or after surgery, and for patients who are not candidates for or do not desire an operation.
Botulinum Toxin
Botulinum toxin (Botox®, Dysport®, Xeomin®, Jeuveau®) temporarily relaxes the muscles that produce dynamic wrinkles. Around the eyes, it softens crow’s feet, smooths the glabellar “11s,” and can subtly elevate the lateral brow when injected with precision. Effects last three to four months. In skilled hands, the result is rested rather than frozen.
Dermal Fillers
Hyaluronic acid fillers restore volume to specific anatomic compartments. Tear trough treatment with thin hyaluronic acid products can dramatically improve dark circles caused by hollowness. Filler can also rebuild brow projection, support the lateral cheek, and soften the temple. Products are reversible with hyaluronidase, providing an important safety margin in this delicate area.
Laser and Energy-Based Resurfacing
Laser and skin rejuvenation treatments address surface concerns — fine lines, pigment, texture, and laxity — that surgery cannot reach. Fractional CO2 and erbium lasers stimulate collagen remodeling and can produce remarkable improvement in crepey lower eyelid skin. Radiofrequency microneedling, intense pulsed light, and chemical peels round out the toolkit.
Non-Surgical Lifting
For patients seeking improvement without an operation, a non-surgical eye lift combines neuromodulator, filler, and energy devices to create a meaningful refresh. This approach has limits — it cannot remove excess skin or herniated fat — but for the right candidate it is transformative.
When Surgery Is Better
- Significant excess upper or lower eyelid skin
- True fat herniation (under-eye bags)
- Brow descent narrowing the visual field
- Festoons unresponsive to other treatment
- Desire for long-lasting, definitive correction
When Non-Surgical Is Better
- Volume loss without skin excess
- Dynamic wrinkles (crow’s feet, glabellar lines)
- Tear trough hollowness without bags
- Skin texture, pigment, or fine line concerns
- Patient prefers gradual or reversible change
Combination Treatment
The most natural and lasting results in periocular rejuvenation almost always come from combining techniques. A patient with upper eyelid hooding, mild brow descent, tear trough hollowness, and crow’s feet should not be offered only blepharoplasty — nor only filler. A thoughtful plan layers solutions to address each anatomic problem.
A Typical Comprehensive Plan
Consider a 55-year-old patient who reports looking tired. On examination she has:
- Mild lateral brow descent
- Upper eyelid dermatochalasis
- Lower eyelid fat herniation with tear trough hollowing
- Crow’s feet at rest and with smiling
- Crepey lower eyelid skin
A combined plan might include a small brow lift, upper blepharoplasty, transconjunctival lower blepharoplasty with fat repositioning, fractional laser resurfacing of the lower lids at the same operative session, and botulinum toxin to the crow’s feet four weeks after surgery. Six months later, a small amount of filler may refine residual asymmetries.
| Concern | Best-Matched Treatment |
|---|---|
| Upper lid hooding | Upper blepharoplasty ± brow lift |
| Under-eye bags | Lower blepharoplasty with fat repositioning |
| Tear trough hollow only | Hyaluronic acid filler or fat grafting |
| Crow’s feet | Botulinum toxin ± laser resurfacing |
| Crepey eyelid skin | Fractional laser or chemical peel |
| Brow descent | Brow lift or precise botulinum toxin |
| Temple or brow deflation | Filler or fat grafting |
Curious which layer of treatment fits your goals best? Explore the Non-Surgical Eye Lift page or read about Upper Facial Aging for a deeper anatomic perspective.
Why an Oculoplastic Surgeon
The periocular region is unique. It contains the most delicate skin on the body, the structures responsible for vision, and an aesthetic centerpiece of the face. Operating here demands more than aesthetic instinct — it requires a deep understanding of eyelid anatomy, tear film physiology, ocular surface health, and the consequences of even millimeter-scale changes in lid position.
Oculoplastic surgeons are ophthalmologists who complete an additional two-year ASOPRS fellowship dedicated exclusively to the eyelids, orbit, and lacrimal system. Their training includes thousands of eyelid surgeries — both reconstructive and cosmetic. They are the specialists called upon to repair complications from cosmetic eyelid surgery performed by others.
The Functional Advantage
An aggressive blepharoplasty can cause chronic dry eye, lagophthalmos (inability to close the eye), lower lid retraction, or even vision-threatening corneal exposure. Oculoplastic surgeons are trained to recognize patients at risk for these complications — pre-existing dry eye, prominent globe anatomy, lower lid laxity — and to modify technique accordingly. They are also the specialists who treat conditions like ptosis and eyelid laxity, which often coexist with cosmetic complaints and may need to be addressed simultaneously.
The Aesthetic Advantage
Because oculoplastic surgeons devote their entire career to this small region, they develop an unusually refined eye for periocular proportion, symmetry, and natural shape. They also command the full range of treatments — surgical and non-surgical — rather than reaching for a single tool.
Recovery and Results
Recovery from periocular rejuvenation depends heavily on which treatments are combined. Non-surgical treatments have minimal downtime; surgery requires a more structured recovery.
Non-Surgical Recovery
Botulinum toxin produces no meaningful downtime — patients return to normal activity immediately and see results within 5 to 14 days. Filler may produce mild swelling and occasional bruising lasting a few days. Laser resurfacing recovery varies with depth: superficial treatments cause two to three days of pinkness, while deeper fractional treatments require five to seven days of social downtime.
Surgical Recovery
After blepharoplasty, patients can expect:
- Days 1–3: Bruising and swelling peak. Cold compresses, head elevation, and rest are essential.
- Days 4–7: Sutures are removed (when used). Swelling improves significantly.
- Week 2: Most patients are comfortable returning to work and social activities.
- Weeks 3–6: Residual subtle swelling resolves. Makeup can camouflage any lingering bruising.
- Months 3–6: Final result settles. Incisions continue to fade.
Longevity of Results
Surgical results are long-lasting. Upper blepharoplasty results commonly persist 10 to 15 years or longer. Lower blepharoplasty with fat repositioning often does not need to be repeated. Brow lifts last 7 to 10 years on average. Non-surgical treatments require ongoing maintenance: botulinum toxin every 3 to 4 months, fillers every 9 to 18 months depending on product and location, and lasers in periodic series.
Important: Aging does not stop after rejuvenation. The treated tissues will continue to age — just from a more refreshed starting point. Sun protection, smoking cessation, and good skin care meaningfully extend results.
Realistic Expectations
The goal of well-executed periocular rejuvenation is not to make a patient look 25 again. It is to make them look like a rested, healthy, well-cared-for version of themselves. Friends should notice that you look refreshed without being able to identify what changed. Done well, periocular rejuvenation is one of the most quietly transformative things modern facial aesthetics can offer.
Take the Next Step
Periocular rejuvenation is highly individualized. The right plan for you depends on your anatomy, your concerns, your tolerance for downtime, and your goals. A consultation with a fellowship-trained oculoplastic surgeon is the best place to begin. To find a qualified special
Frequently Asked Questions
- Who is a good candidate for periocular rejuvenation?
- Ideal candidates are generally healthy individuals with concerns about aging around the eyes, such as drooping lids, under-eye bags, or loss of volume, who have realistic expectations about outcomes. Good candidates should have no active eye infections or serious medical conditions that would interfere with healing. A thorough consultation with a fellowship-trained oculoplastic surgeon will determine if you're a suitable candidate based on your specific concerns and anatomy.
- What should I expect during my initial consultation?
- During your consultation, the surgeon will examine the skin, eyelids, and surrounding structures to assess your concerns and develop a customized treatment plan. They will discuss your goals, review before-and-after photos, and explain which surgical or non-surgical options would best address your needs. You'll also receive information about risks, recovery, and realistic outcomes so you can make an informed decision.
- How long do the results from periocular rejuvenation last?
- Surgical results, such as those from blepharoplasty or midface lifting, are generally long-lasting and can continue to look natural for many years. Non-surgical components, like injectables or laser treatments, typically require maintenance appointments every 6-12 months to sustain results. The longevity of your results depends on your age, skin quality, sun exposure, and lifestyle factors.
- What are the potential risks and complications?
- As with any surgical procedure, potential risks include temporary swelling, bruising, dry eyes, and asymmetry, though serious complications are rare when performed by experienced surgeons. Specific risks may vary depending on which procedures are recommended for you. Your surgeon will discuss all potential complications during your consultation and explain how they minimize these risks through their surgical expertise.
- What does post-operative care involve?
- Post-operative care typically includes using prescribed eye drops, applying cold compresses, avoiding strenuous activity for 1-2 weeks, and protecting your eyes from sun exposure. You'll have scheduled follow-up visits to monitor healing and address any concerns. Most patients can return to light activities within a week and resume normal routines within 2-3 weeks, depending on the extent of treatment.
- Is periocular rejuvenation covered by insurance?
- Most cosmetic periocular rejuvenation procedures are not covered by insurance since they're elective. However, if a procedure addresses a functional problem—such as eyelid ptosis affecting vision—some insurance plans may cover that portion. It's best to discuss costs and potential insurance coverage with your surgeon's office before scheduling your procedure.
- When should I see a fellowship-trained oculoplastic surgeon instead of a general plastic surgeon?
- A fellowship-trained oculoplastic surgeon has specialized expertise in the delicate anatomy around the eyes and is uniquely qualified to achieve natural-looking results while preserving eye function. They're trained to manage complex cases and potential complications specific to the periocular area. For comprehensive rejuvenation involving the eyelids and surrounding structures, an oculoplastic specialist is the ideal choice.
Find a Specialist
Connect with a board-certified oculoplastic surgeon who specializes in periocular rejuvenation.
Search the Directory →