Lacrimal System
Treatment of blocked tear ducts, chronic tearing, dacryocystorhinostomy (DCR), and lacrimal infections — adult and pediatric.
Patient Education Video
A complete overview of lacrimal anatomy, blocked tear duct causes, and surgical treatment options including probing, DCR, and endoscopic DCR.
Lacrimal System — Interactive Surgical Animation
Explore lacrimal anatomy and surgical treatments including probing, silicone intubation, DCR, and CDCR using the menu on the left.
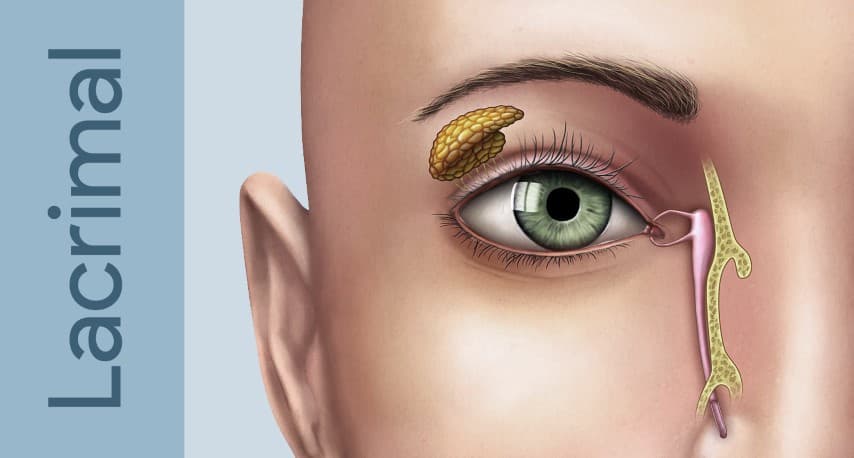
The Lacrimal System
The lacrimal system produces, distributes, and drains tears. A healthy tear film is essential for corneal health, clear vision, and comfort. When any part of the drainage pathway is blocked, tears overflow onto the cheek (epiphora), stagnate in the drainage sac, and become a reservoir for infection.
How Tears Drain
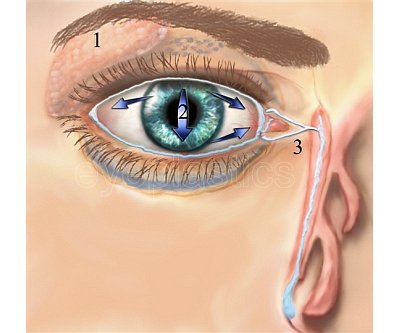
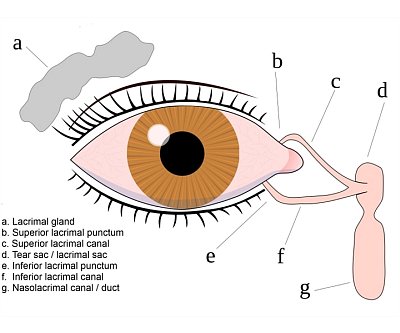
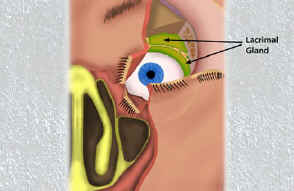
- The lacrimal gland (upper outer orbit) and accessory glands produce the aqueous tear layer
- Blinking sweeps tears medially toward the inner corner of the eye
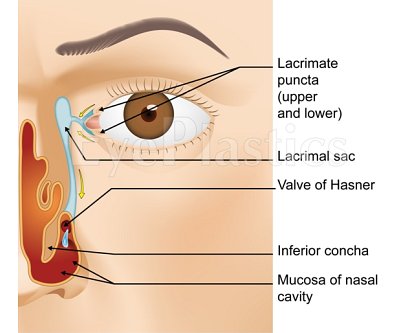
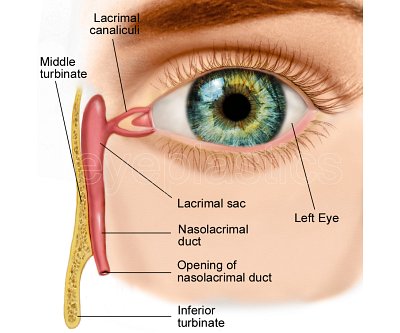
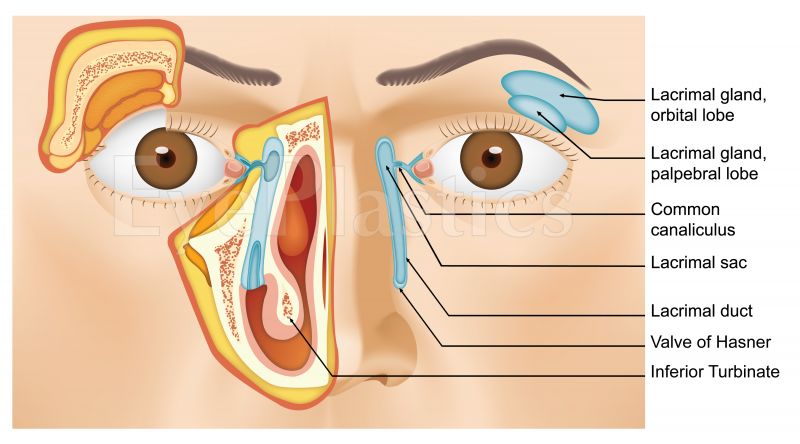
- Tears enter the puncta (small openings at the inner corner of each eyelid), travel through the canaliculi, and collect in the lacrimal sac
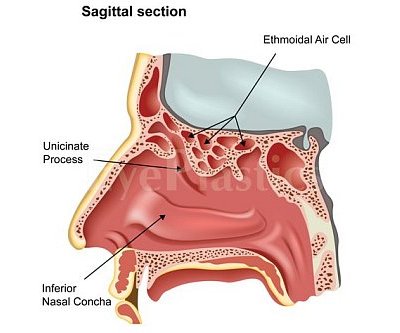
- From the sac, tears drain through the nasolacrimal duct and exit under the inferior turbinate in the nose (valve of Hasner)
Symptoms of Obstruction
- Excessive tearing (tears spilling over the eyelid margin — epiphora)
- Mucous or purulent discharge, especially in the morning
- Recurrent red eye or conjunctivitis
- Painful, swollen inner corner of the eyelid (acute dacryocystitis)
- Secondary skin changes or maceration of the lower lid skin
For a detailed overview of lacrimal anatomy, see the Anatomy Overview or the dedicated Lacrimal Anatomy page.
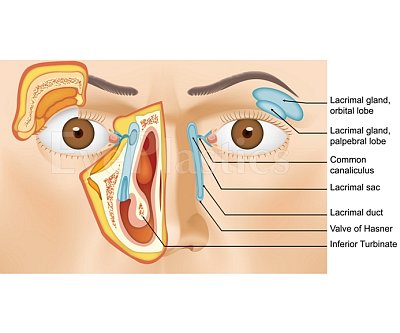
Lacrimal Anatomy
Understanding the anatomy guides both the diagnostic work-up and the choice of surgical repair. The drainage system has several potential sites of obstruction:
- Punctal stenosis: the opening is too small or closed; common in elderly patients and after topical medication use
- Canalicular obstruction: the canaliculi (upper and lower) may be scarred by infection, trauma, or chemotherapy agents (especially 5-FU and docetaxel)
- Common canalicular obstruction: where the upper and lower canaliculi join before entering the lacrimal sac
- Nasolacrimal duct obstruction (NLDO): the most common site; the duct narrows or occludes at or just above the valve of Hasner
Evaluation of Tearing
A systematic evaluation identifies the site and severity of obstruction before planning treatment.
History
- Duration and laterality of tearing
- Associated discharge, pain, or swelling over the lacrimal sac
- Prior eye surgery, chemotherapy, or topical medication use (especially anti-glaucoma drops)
- History of facial trauma, nasal surgery, or chronic sinusitis
- Prior episodes of dacryocystitis
Clinical Tests
- Dye disappearance test (DDT): fluorescein dye placed in both eyes; persistence of dye on slit lamp after 5 minutes indicates delayed drainage. Quantified by asymmetry between eyes
- Jones I test (primary dye test): cotton swab placed beneath the inferior turbinate; recovery of fluorescein confirms functional patency of the entire system
- Jones II test (secondary dye test): if Jones I is negative, the sac is irrigated with clear saline; recovery of fluorescein-stained fluid from the nose confirms partial obstruction at or below the sac
- Lacrimal irrigation / probing: a fine cannula irrigates the system through the punctum. Hard stop (probe contacts bone) indicates a patent canaliculus; soft stop (probe meets resistance before bone) suggests canalicular stenosis. Reflux of fluid indicates nasolacrimal obstruction
- Regurgitation test: pressure over the lacrimal sac expresses mucoid or purulent material through the punctum — confirms an obstructed, infected sac (dacryocystitis)
Imaging
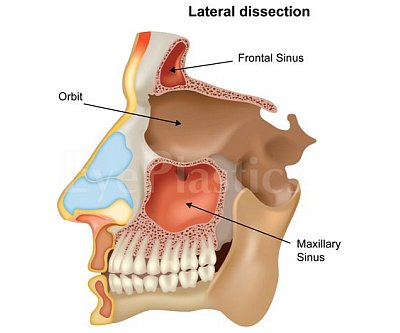
- CT scan of orbits and sinuses: identifies bony anatomy, nasolacrimal canal dimensions, and sinus pathology; essential before revision DCR surgery
- Dacryocystography (DCG): contrast injected into the system outlines the anatomy and identifies the level of obstruction
- Nasal endoscopy: evaluates the nasal cavity, inferior meatus, and valve of Hasner; identifies intranasal pathology (polyps, deviated septum) that may contribute to obstruction
Congenital Nasolacrimal Duct Obstruction
Congenital NLDO is one of the most common conditions seen in infants, occurring in approximately 6% of newborns. In most cases, the duct fails to fully canalize at its distal end (valve of Hasner) before birth, leaving a thin membrane blocking tear drainage.
| Presentation | Features |
|---|---|
| Simple obstruction | Epiphora, mucopurulent discharge; most resolve spontaneously |
| Congenital fistula | Abnormal opening in the skin below the medial canthus; may drain tears externally |
| Dacryocele / mucocele | Bluish, tense swelling at the medial canthus at birth from amniotic fluid trapped in an obstructed sac; may require urgent probing |
| Acute neonatal dacryocystitis | Infection of the lacrimal sac in the first weeks of life; risk of orbital cellulitis; requires prompt antibiotics and probing |
Natural History & Management
- Spontaneous resolution: approximately 90% of cases resolve by age 12 months as the duct canalizes naturally. Watchful waiting with lacrimal massage is appropriate until this age
- Lacrimal sac massage (Crigler technique): firm downward pressure over the lacrimal sac 2–3 times daily can create a hydrostatic pressure wave that opens the membrane at the valve of Hasner. Topical antibiotics treat secondary infection but do not cure the obstruction
Surgical Treatment — When Massage Fails
- Office probing (age 6–12 months): A fine probe is passed through the punctum and nasolacrimal duct under topical anesthesia in the office. Success rate ≈ 90% in the first year of life. Success rate declines with advancing age as the membrane thickens
- Probing under general anesthesia (age 12–24 months): Performed if office probing fails or is deferred past age 12 months; often combined with silicone intubation
- Silicone intubation: A silicone tube is threaded through both puncta, down through the duct, and retrieved from the nose. Held in place for 3–6 months to prevent re-stenosis. Success rate >90% when added to probing
- Balloon dacryoplasty: A fine balloon catheter is inflated at 75–150 PSI within the duct to dilate the obstruction. Alternative to intubation for refractory cases
- DCR (dacryocystorhinostomy): Reserved for failures of probing and intubation, or when anatomy (severe stenosis, canalicular disease) precludes simpler approaches. Success rates comparable to adult DCR
Acquired Nasolacrimal Duct Obstruction
Acquired NLDO is divided into primary (PANDO — idiopathic, inflammatory/fibrotic) and secondary (SALDO — a specific identifiable cause).
Primary PANDO
PANDO is the most common acquired NLDO in adults, predominantly affecting middle-aged to elderly women. Progressive fibrosis and epithelial loss narrow the nasolacrimal canal, likely related to reduced estrogen levels affecting the nasolacrimal mucosa (analogous to osteoporosis). The bony canal dimensions are measurably smaller in affected women.
Secondary SALDO — Causes
- Infectious: Actinomyces, Propionibacterium (cause dacryoliths/stones), herpes simplex virus (canalicular scarring), fungal (Aspergillus, Candida)
- Inflammatory: Wegener’s granulomatosis, sarcoidosis, cicatricial pemphigoid, inflammatory bowel disease
- Neoplastic: lacrimal sac tumors (usually present with bloody epiphora), nasal or sinus tumors extending to the duct
- Traumatic / iatrogenic: nasal surgery, overly aggressive probing, facial fractures, orbital decompression surgery
- Medications: topical anti-glaucoma drops (especially epinephrine and idoxuridine), systemic docetaxel or 5-FU chemotherapy causing canalicular fibrosis
- Mechanical: dacryoliths (calcified concretions), rhinoliths, mucoceles compressing the duct from outside
Infections of the Lacrimal System
Dacryoadenitis (Lacrimal Gland Infection)
- Inflammation or infection of the lacrimal gland in the superolateral orbit
- Acute: bacterial (Staphylococcus, Streptococcus) or viral (EBV, mumps, CMV, VZV); painful S-shaped lid deformity; treat with systemic antibiotics or antivirals
- Chronic: associated with systemic disease — sarcoidosis, Sjögren’s syndrome, lymphoma, IgG4-related disease; biopsy of the lacrimal gland is often required to establish diagnosis
Canaliculitis
Canaliculitis is infection of the canaliculus (the channel connecting the punctum to the lacrimal sac). It is commonly misdiagnosed and undertreated — always consider it when a patient has a “chronic conjunctivitis” of one eye that fails to respond to drops.
- Most common cause: Actinomyces israelii (80% of cases); the organism forms sulphur granules (concretions) within the canaliculus
- Other causes: Propionibacterium, Fusobacterium, Candida, Aspergillus, herpes simplex
- Classic signs: unilateral red eye, mucopurulent discharge, swollen pouting punctum (the “lacrimal pouch sign”); yellow concretions expressed from the punctum on compression
- Diagnosis: clinical — probe passes easily but with a “gritty” sensation; microscopy and culture of expressed material confirms organism
- Treatment: canaliculotomy (incision of the canaliculus through its posterior wall) with curettage of concretions, followed by irrigation with penicillin or povidone-iodine. Topical antibiotics alone almost always fail. Incomplete concretion removal leads to recurrence
Dacryocystitis — Acute

Acute dacryocystitis is a bacterial infection of the lacrimal sac, almost always arising from nasolacrimal duct obstruction with stasis of tears and secondary infection.
- Presentation: sudden-onset pain, redness, and tender swelling at the medial canthus below the medial canthal tendon (this location distinguishes dacryocystitis from ethmoid sinusitis or subcutaneous abscess, which present above or along the tendon)
- Common organisms: Staphylococcus aureus (most common), Streptococcus pneumoniae, Haemophilus influenzae, gram-negative rods in immunocompromised patients
- Treatment:
- Oral antibiotics (Augmentin, Keflex) for mild-to-moderate cases
- IV antibiotics (nafcillin, vancomycin for MRSA coverage) for severe disease, periorbital spread, or failure of oral therapy
- Warm compresses
- Do not probe an acutely infected system — probing risks spreading infection and creating a fistula
- Incision and drainage if abscess forms and is fluctuant
- DCR surgery after the acute infection resolves (typically 4–6 weeks later) to prevent recurrence
- Complications if untreated:
- Preseptal (periorbital) cellulitis
- Orbital cellulitis and abscess (sight- and life-threatening)
- Lacrimal fistula (spontaneous drainage through the skin)
- Mucocele (chronic distended, obstructed sac without acute infection)
- Cavernous sinus thrombosis (rare but potentially fatal)
Dacryocystitis — Chronic
- A chronically obstructed lacrimal sac that is distended with mucoid or mucopurulent fluid with minimal acute inflammation
- Presents as recurrent episodes of mild discharge and epiphora, with a soft, compressible swelling at the medial canthus
- Pressure on the sac expresses mucoid material through the punctum (regurgitation test positive)
- May harbor dacryoliths (stones) from Actinomyces or Candida species
- Treatment: DCR surgery; topical antibiotics provide only temporary symptomatic relief
Surgical Treatment
The goal of lacrimal surgery is to restore or create a functional tear drainage pathway from the lacrimal sac into the nasal cavity. The approach depends on the site and extent of obstruction, prior surgery, and nasal anatomy.
1. Probing & Irrigation
- First-line for congenital NLDO after failed conservative management
- Lacrimal probe passed through punctum into the nasolacrimal duct under topical or general anesthesia
- Success rate: ≈ 90% in infants under 12 months; declines with age
- Often combined with silicone intubation to prevent re-stenosis
2. Balloon Dacryoplasty
- Deflated balloon catheter (LacriCATH®) inserted into the nasolacrimal duct; inflated at 75 PSI for 90 seconds at two positions within the duct
- Alternative to intubation for refractory congenital NLDO and some adult cases of functional stenosis
- Minimal scarring; performed under general anesthesia
3. Endoscopic DCR (Dacryocystorhinostomy)
Endoscopic DCR is the preferred approach for acquired NLDO in adults, chronic dacryocystitis, and failed probing with intubation in children. A new bony window is created between the lacrimal sac and the nasal cavity under direct endoscopic visualization, bypassing the blocked nasolacrimal duct entirely.
Step-by-Step Procedure
- Anesthesia: General anesthesia (standard) or local anesthesia with IV sedation. Topical vasoconstrictors applied intranasally
- Nasal access: Endoscope introduced through the nostril; middle turbinate reflected to expose the lateral nasal wall adjacent to the lacrimal bone
- Lacrimal sac identification: Fine probe passed through the punctum transilluminates the sac through the nasal mucosa for precise localization
- Bony ostium creation: Nasal mucosa elevated; lacrimal bone and anterior maxilla removed with powered instrumentation (microdebrider and Kerrison rongeur) to create a 10–12 mm bony opening into the lacrimal sac
- Mucosal flap: Nasal mucosa fashioned into flaps to line the new anastomosis and promote primary healing
- Sac marsupialization: Lacrimal sac opened and apposed to nasal mucosa to create a wide, epithelialized rhinostomy
- Silicone stent: Bicanalicular silicone tube threaded from each punctum through the rhinostomy and retrieved nasally; removed in clinic at approximately 3 months
- Closure: Absorbable nasal packing; no skin incision; no external scar
Recovery
- Same-day outpatient procedure; home the same day
- Oral antibiotics, antibiotic eye drops, and nasal saline sprays for 2 weeks
- Avoid nose blowing for 2 weeks; expect mild bloody nasal discharge for several days
- Success rate: 85–95% resolution of tearing
4. External DCR
- Incision at the medial canthus; direct access to the lacrimal sac and nasolacrimal duct
- Preferred when intranasal anatomy (tumors, severe deviation, prior sinus surgery) prevents an endoscopic approach, or when lacrimal sac biopsy is needed for suspected tumor
- Success rate comparable to endoscopic DCR; small external scar hides in the nasofacial groove and is rarely noticeable
- Silicone stent placed and removed at 3 months
5. CDCR / Jones Tube
When the canalicular system is too scarred or absent to use (severe canalicular stenosis, canalicular trauma, failed multiple DCRs), a Jones tube (Pyrex glass bypass tube) is implanted to create a direct channel from the inner corner of the eye to the nasal cavity.
- The tube bypasses the entire canalicular and sac system
- Permanent implant; requires long-term follow-up to monitor tube position and patency
- Tubes may require adjustment or replacement over time
- Patients must be able to occlude the tube with the finger to blow the nose
Lacrimal Trauma — Canalicular Lacerations

Canalicular lacerations occur when trauma to the medial eyelid severs the canaliculus. Because the canaliculus lies just beneath the skin medial to the punctum, even seemingly superficial medial eyelid lacerations frequently involve it. If not repaired promptly and correctly, permanent epiphora results.
Recognition
- Any laceration medial to the punctum should be assumed to involve the canaliculus until proven otherwise
- Common mechanisms: dog bites (very high frequency of canalicular involvement), fist injury, motor vehicle accident, fishhook
- The lower canaliculus is injured more commonly than the upper
- Both canaliculi may be involved if trauma crosses both lids
Repair Principles
Canalicular repair must be performed within 24–48 hours for best results. The key steps:
- Identify both ends of the lacerated canaliculus under magnification (surgical microscope or loupes)
- Place a stent (silicone tube) to maintain the lumen during healing and prevent stricture
- Reapproximate the canalicular ends over the stent with fine absorbable sutures (7-0 Vicryl or 8-0 Vicryl)
- Repair the eyelid in layers
Stent Options
- Monocanalicular stent (Mini-Monoka): stent placed only in the injured canaliculus; plugs at the punctum; avoids potential damage to the normal canaliculus. Preferred for isolated lower canalicular laceration
- Bicanalicular stent: looped through both upper and lower canaliculi; retrieved nasally. Required when the common canaliculus or lacrimal sac is involved. Disadvantage: potential trauma to the uninvolved canaliculus
- Stents removed at 3–6 months
Success Rate
- Prompt, meticulous primary repair achieves functional patency in approximately 85–90% of cases
- Delayed repair or failure of initial repair may require DCR or ultimately Jones tube if the canaliculus cannot be reconstructed
Frequently Asked Questions
- What causes a blocked tear duct?
- The most common cause in adults is involutional stenosis — gradual narrowing of the nasolacrimal duct with age. Other causes include infection (dacryocystitis), trauma, nasal or sinus surgery, certain eye drops (glaucoma medications), and inflammatory diseases. In infants, blocked tear ducts are usually due to a membrane at the lower end of the duct that fails to open at birth.
- What is DCR surgery?
- Dacryocystorhinostomy (DCR) is the surgical bypass of a blocked nasolacrimal duct. A new drainage opening is created directly between the lacrimal sac and the nasal cavity, bypassing the blocked duct entirely. DCR can be performed externally (through a small incision beside the nose) or endoscopically (through the nose, with no external incision).
- What is the success rate of DCR surgery?
- External DCR has long-term success rates of approximately 90–95%. Endoscopic DCR has similar success rates in experienced hands. Most patients experience complete relief of tearing after surgery.
- Can a child's blocked tear duct resolve without surgery?
- Yes — up to 90% of congenital nasolacrimal duct obstructions in infants resolve spontaneously by 12 months with massage and topical antibiotics for infections. If the obstruction persists at 12–18 months, a simple probing procedure is performed under brief anesthesia.
- What should I expect during my lacrimal system consultation?
- During your consultation, your oculoplastic surgeon will review your symptoms, examine your eyes and tear drainage system, and may perform diagnostic tests such as dye tracing or imaging to identify the exact location and cause of the blockage. They will discuss your treatment options, explain the recommended procedure, and answer any questions about what to expect before and after treatment. This appointment helps ensure you're a good candidate for surgery and allows you to make an informed decision about your care.
- What is the recovery timeline after lacrimal surgery?
- Most patients experience some mild discomfort, swelling, and drainage for the first 1-2 weeks following lacrimal surgery. You can typically return to light activities within a few days, though strenuous exercise and heavy lifting should be avoided for 2-3 weeks to prevent complications. Complete healing of the surgical site takes several weeks, and your surgeon will provide specific instructions on eye drops, nasal saline rinses, and activity restrictions to support proper healing.
- Are there risks or complications associated with lacrimal surgery?
- Like any surgical procedure, lacrimal surgery carries some risks, including infection, bleeding, and temporary or persistent tearing. In rare cases, the surgical site may scar and narrow over time, requiring revision surgery. Your surgeon will discuss all potential complications during your consultation and explain how they minimize these risks through advanced surgical techniques and proper post-operative care instructions.
Find a Specialist
Connect with a board-certified oculoplastic surgeon who specializes in lacrimal system.
Search the Directory →