
Symblepharon
Surgical repair of symblepharon — conjunctival adhesions from chemical burns, Stevens-Johnson syndrome, and cicatrizing conjunctivitis — with mucous membrane and amniotic membrane grafting.
What is Symblepharon
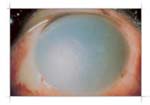
Symblepharon is an adhesion between the palpebral conjunctiva (lining the inner eyelid) and the bulbar conjunctiva (covering the eye surface). These bands of scar tissue tether the eyelid to the eyeball, restricting eyelid movement, limiting ocular motility, and distorting the conjunctival fornix — the recessed pocket where the eyelid lining meets the eye. In severe cases, symblepharon obliterates the fornix entirely (ankyloblepharon), causing functional blindness.
Symblepharon is most commonly caused by severe chemical injury to the eye. Related conditions include Eyelid Laxity and Lagophthalmos, which may coexist when eyelid scarring accompanies symblepharon.
Causes
Symblepharon results from any condition that damages both the palpebral and bulbar conjunctival surfaces simultaneously, allowing them to fuse during healing:
- Chemical burns — alkali burns (lye, ammonia, cement) are most severe; acid burns produce more limited injury. Alkali penetrates rapidly through the cornea into the anterior chamber, with symblepharon developing as conjunctival surfaces heal together.
- Stevens-Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN) — drug-hypersensitivity reactions causing blistering of mucous membranes including conjunctiva. Symblepharon is a hallmark late sequela of SJS/TEN ocular involvement and may progress over months to years.
- Ocular Cicatricial Pemphigoid (OCP) / Mucous Membrane Pemphigoid — autoimmune subepithelial blistering disease causing progressive conjunctival scarring and shrinkage. Symblepharon formation in OCP follows a characteristic inferior fornix shortening pattern.
- Radiation to the orbit or eye — therapeutic radiation for orbital or periocular tumors causes progressive conjunctival fibrosis.
- Severe conjunctival infections — trachoma (Chlamydia trachomatis) is the leading infectious cause of symblepharon worldwide, particularly in developing countries. Recurrent infections cause progressive conjunctival scarring.
- Trauma — perforating injuries or severe blunt trauma with conjunctival laceration.
- Post-surgical scarring — prior conjunctival surgery, enucleation, or orbital procedures.
- Linear IgA disease and other cicatrizing conjunctivitides
Clinical Staging
Symblepharon severity is graded by the degree of fornix obliteration:
- Grade I: Partial symblepharon — adhesive bands present, forniceal depth reduced but some fornix preserved
- Grade II: Moderate symblepharon — fornix significantly shortened, motility restricted
- Grade III: Severe symblepharon — fornix nearly obliterated, eyelid movement markedly restricted
- Grade IV (Ankyloblepharon): Complete adhesion — eyelid fused to globe, no identifiable fornix
Associated findings include keratinization of the conjunctiva, limbal stem cell deficiency (LSCD) causing corneal vascularization and opacification, and trichiasis from distorted lid margin.
Acute Phase Management
The goal in the acute phase of chemical injury or SJS is to prevent symblepharon formation:
- Immediate copious irrigation — for chemical burns, continuous saline or water irrigation for 30–60 minutes to remove the offending agent; target conjunctival pH 7.0–7.3.
- Symblepharon ring / conformer — a smooth ring or conformer device placed in the fornix to physically separate palpebral and bulbar surfaces during healing. Must be maintained continuously and removed only for medication instillation.
- Fornix sweeping — gentle blunt dissection of early adhesions with a glass rod or spatula, performed daily or multiple times per day in the acute phase under topical anesthesia.
- Amniotic membrane transplantation (AMT) — suturing or gluing amniotic membrane (AM) to the ocular surface in the acute phase of chemical burns or SJS significantly reduces symblepharon formation, promotes re-epithelialization, and reduces inflammation. Both sutured and ProKera® ring-mounted AM devices are used.
- Topical cyclosporine and corticosteroids — to reduce conjunctival inflammation in acute SJS/OCP.




Surgical Treatment of Established Symblepharon
Once symblepharon has matured, surgical lysis and fornix reconstruction are required to restore motility and eyelid function. Surgery is indicated for:
- Restricted ocular motility causing diplopia
- Fornix shortening preventing prosthetic fitting (in anophthalmos)
- Trichiasis from distorted lid margin abrading the cornea
- Functional limitations from eyelid restriction
Mucous Membrane Grafting (MMG)
After surgical lysis of the symblepharon bands, the raw surfaces must be covered with a graft to prevent re-adhesion. Autologous mucous membrane (from buccal mucosa, nasal septum, or hard palate) is harvested and sutured to line the reconstructed fornix. MMG provides a durable, non-keratinizing surface.
Amniotic Membrane Grafting
Amniotic membrane can be used as an adjunct or alternative to autologous mucous membrane for fornix reconstruction. It provides anti-inflammatory, anti-fibrotic, and anti-angiogenic properties, promoting re-epithelialization. Often combined with a conformer to maintain fornix depth post-operatively.
Limbal Stem Cell Transplantation
When symblepharon is accompanied by limbal stem cell deficiency — evidenced by corneal vascularization, conjunctivalization of the cornea, and recurrent epithelial breakdown — limbal stem cell transplantation (LSCT) is necessary before or concurrent with symblepharon repair to restore a stable corneal surface. Sources include:
- Autologous LSCT (CLAU/CLET) — from the fellow unaffected eye; avoids immunosuppression
- Allogeneic LSCT (KLAL/CLET) — from cadaveric donor tissue; requires systemic immunosuppression
- Ex vivo expanded limbal cells (CLET) — cultured on amniotic membrane carrier; now available at specialized centers
Post-operative Conformer Use
A conformer or custom ocular prosthesis is placed immediately after fornix reconstruction and maintained to prevent re-adhesion during healing. In progressive cicatrizing conditions (OCP), the conformer may need to be worn indefinitely.
Systemic Disease Management
In autoimmune cicatrizing conjunctivitis (OCP, SJS), treatment of the underlying systemic disease is essential to halt progression:
- OCP: Dapsone (first-line), methotrexate, cyclophosphamide, or rituximab. Surgery should not be performed on actively inflamed OCP eyes — inflammation accelerates scarring.
- SJS: Cyclosporine, etanercept, or intravenous immunoglobulin in the acute phase may reduce severity. Long-term management focuses on ocular surface rehabilitation.
Oculoplastic management of symblepharon is most effective when performed in collaboration with rheumatology, dermatology, or immunology for systemic disease control.
Frequently Asked Questions
- What is symblepharon?
- Symblepharon is an adhesion (scarring) between the conjunctiva of the eyelid and the conjunctiva of the eyeball. It restricts eye movement, causes chronic irritation, and can impair vision. It is caused by cicatrizing (scarring) conditions including chemical burns, Stevens-Johnson syndrome (SJS), ocular cicatricial pemphigoid, and severe ocular infections.
- How is symblepharon treated?
- Acute cases require aggressive lubrication and, in chemical burns, immediate irrigation and amniotic membrane placement to prevent adhesion formation. Established symblepharon is released surgically, with conjunctival defects reconstructed using mucous membrane grafts (from the inner lip) or amniotic membrane transplantation. Recurrence prevention is critical.
- Am I a good candidate for symblepharon surgery?
- Candidates for symblepharon repair typically have significant conjunctival scarring from chemical burns, Stevens-Johnson syndrome, or chronic cicatrizing conditions that limit eye movement or cause discomfort. Your oculoplastic surgeon will evaluate the extent of your adhesions, overall eye health, and tear production to determine if you're a suitable candidate. Generally, surgery is recommended when the condition affects vision, eye comfort, or your ability to wear contact lenses or glasses.
- What should I expect during my initial consultation?
- During your consultation, your surgeon will perform a comprehensive eye examination, including assessment of eye mobility, tear film quality, and the extent of conjunctival adhesions. They will review your medical history, discuss what caused your symblepharon, and explain the surgical approach tailored to your specific situation. You'll have the opportunity to ask questions and discuss realistic outcomes, recovery time, and any concerns about the procedure.
- What happens after symblepharon surgery?
- After surgery, you'll need to follow specific post-operative care instructions, which may include using prescribed eye drops, keeping the eye clean, and avoiding strenuous activities for several weeks. Regular follow-up visits are essential to monitor healing, ensure the grafted tissue is integrating properly, and manage any inflammation. Your surgeon may recommend protective eyewear or specialized contact lenses to prevent re-adhesion during the critical healing period.
- What are the potential risks and complications of this surgery?
- While symblepharon repair is generally safe, potential risks include graft failure, re-scarring or re-adhesion of the conjunctiva, infection, and inflammation. Some patients may experience temporary discomfort, tearing, or light sensitivity during healing. Serious complications are uncommon when the procedure is performed by a fellowship-trained oculoplastic surgeon and post-operative care instructions are carefully followed.
- How long do the results of symblepharon surgery last?
- Many patients experience long-lasting improvement in eye mobility and comfort after symblepharon repair, though the longevity of results depends on the severity of the original condition and how well the tissue heals. Some patients may require additional procedures if re-scarring occurs, as the eye's natural healing response can sometimes lead to recurrent adhesions. Your surgeon will discuss realistic expectations and develop a long-term management plan to maintain your results.
Find a Specialist
Connect with a board-certified oculoplastic surgeon who specializes in symblepharon.
Search the Directory →