
Lasers
Laser skin resurfacing (CO₂, Er:YAG, fractional), vascular lasers, IPL, and pigment lasers for periorbital and facial rejuvenation.
Laser Skin Treatments — Overview
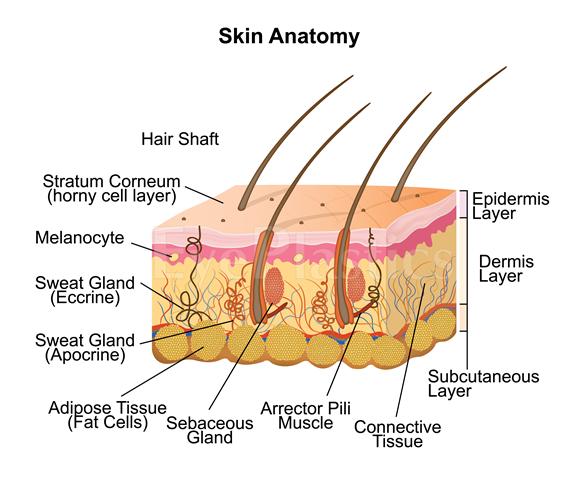
Lasers and energy-based devices use precisely controlled light or electromagnetic energy to remodel, resurface, and rejuvenate skin. Oculoplastic surgeons use these modalities to treat periorbital and facial skin concerns including wrinkles, sun damage, pigmented lesions, vascular lesions, and acne scars. Laser treatments are often combined with surgical procedures for comprehensive periorbital rejuvenation.
Laser treatments complement surgical eyelid procedures — see Blepharoplasty and Brow Lift. For non-laser skin treatments, see Skin Rejuvenation. For rosacea-related vascular laser treatment, see Rosacea.
Ablative Laser Resurfacing
Ablative lasers vaporize the outer layers of skin — the epidermis and superficial dermis — allowing new skin to regenerate with improved texture, tone, and reduced wrinkles. Significant collagen remodeling occurs as the skin heals, producing skin-tightening effects that continue for months after the procedure. Ablative resurfacing provides the most dramatic improvement of any energy-based treatment.
CO₂ Laser (Carbon Dioxide) — The Gold Standard
- Wavelength: 10,600 nm — strongly absorbed by water in skin tissue, producing precise ablation
- Depth: Deepest ablative penetration; treats significant photoaging and deep periorbital rhytids
- Best for: Deep wrinkles around the eyes and mouth, actinic (sun) damage, skin texture irregularities, actinic keratoses
- Recovery: 10–14 days of weeping, crusting, and raw skin; pink/red color persists 1–3 months; full healing 3–6 months
- Results: Dramatic — up to 50% reduction in wrinkle depth; significant improvement in skin texture and tone
- Risks: Prolonged erythema, hypopigmentation (loss of skin color — permanent in some cases), hyperpigmentation (especially in darker skin), scarring, ectropion of the lower eyelid (from excessive ablation near the lid margin), infection
- Patient selection: Best for Fitzpatrick skin types I–III; use with caution in types IV; avoid in types V–VI
Er:YAG Laser (Erbium:YAG)
- Wavelength: 2,940 nm — more selective water absorption than CO₂; minimal thermal damage to adjacent tissue
- Depth: More superficial ablation than CO₂; less thermal spread
- Best for: Mild-to-moderate photoaging, fine lines, superficial pigmentation, seborrheic keratoses
- Recovery: 5–7 days; less post-procedural erythema and faster re-epithelialization vs. CO₂
- Advantages over CO₂: Lower risk of prolonged erythema, pigment changes, and scarring; better tolerated in Fitzpatrick types III–IV
- Limitation: Less collagen remodeling and skin tightening than CO₂
Fractional Laser Resurfacing
Fractional technology revolutionized ablative resurfacing by treating only a fraction of the skin in a grid pattern — creating microscopic columns of treated tissue (microthermal zones) surrounded by untreated skin. The intact surrounding tissue acts as a reservoir for rapid healing, dramatically reducing downtime compared to full-field ablation while still producing meaningful results.
Fractional Ablative
- Fraxel Re:pair® (fractional CO₂), Lumenis ActiveFX/DeepFX
- Creates microscopic ablated columns surrounded by untreated bridges of skin
- Recovery: 3–7 days (vs. 10–14 for full-field CO₂)
- Results: Moderate improvement in one treatment; can be repeated for progressive improvement
- Multiple treatment sessions over months can approach full-ablative results with significantly less downtime
- Lower risk of hypopigmentation and scarring than full-field ablation — better suited to Fitzpatrick types III–IV
Fractional Non-Ablative
- Fraxel Restore® (1550 nm / 1927 nm), Palomar Icon, Clear + Brilliant
- Heats dermal tissue creating controlled micro-injuries without ablating the surface — epidermis remains intact
- Minimal downtime: 1–3 days of swelling, mild redness, and bronzed appearance as treated columns slough
- Best for: Fine lines, textural irregularities, melasma, acne scarring, mild pigmentation — not significant wrinkles or laxity
- Requires a series of 3–5 sessions for meaningful improvement
- Suitable for all Fitzpatrick skin types, including V–VI with proper technique and parameters
Before & After — Laser Skin Rejuvenation






Vascular & Pigment Lasers
Selective photothermolysis — the principle of using wavelengths specifically absorbed by target chromophores (melanin or oxyhemoglobin) — allows targeted treatment of vascular and pigmented lesions with minimal surrounding skin damage:
Pulsed Dye Laser (PDL) — 595 nm
Selectively absorbed by oxyhemoglobin in vessels. First-line treatment for:
- Facial telangiectasias and spider veins
- Port wine stains and hemangiomas
- Rosacea-associated redness
- Erythematous (red) surgical scars
Characteristic post-treatment purpura (bruising) resolves in 7–14 days. Newer "V-beam Perfecta" settings allow treatment without purpura at the cost of some efficacy.
KTP Laser (532 nm) & Nd:YAG (1064 nm)
- KTP (532 nm): Excellent for superficial facial redness and fine telangiectasias; less purpura than PDL
- Long-pulsed Nd:YAG (1064 nm): Penetrates deeper; treats larger vessels, leg veins, and darker-skin vascular lesions with minimal melanin absorption — safer for Fitzpatrick V–VI
Q-Switched / Picosecond Lasers (Pigment)
- Ultra-short pulse durations shatter melanin particles into micro-fragments for elimination
- Q-switched Nd:YAG (1064/532 nm), Alexandrite (755 nm), Ruby (694 nm)
- Picosecond lasers (PicoSure, PicoWay, Enlighten) — shorter pulses (picoseconds vs. nanoseconds) reduce thermal injury, improve efficacy for resistant pigmentation and tattoo removal
- Indications: Lentigines (age spots), ephelides (freckles), melasma (combined with topical treatment), tattoo removal, nevus of Ota
Intense Pulsed Light (IPL)
IPL uses filtered broadband light (not a laser) to target both melanin and oxyhemoglobin simultaneously, treating mixed vascular and pigmented changes from photoaging in a single session. It does not resurface skin but provides significant improvement in overall facial tone, redness, and pigmentation.
- Best for: Diffuse facial redness (rosacea), age spots, freckles, overall photodamage, periocular telangiectasias, meibomian gland dysfunction (therapeutic benefit for dry eye)
- Protocol: Series of 3–5 treatments spaced 3–4 weeks apart; annual maintenance
- Downtime: Minimal — pigmented lesions darken and flake off over 7–14 days; redness resolves in 1–2 days
- Limitations: Not safe for Fitzpatrick types V–VI due to melanin competition; not suitable for deeply pigmented lesions
Skin Type & Treatment Selection
The Fitzpatrick phototyping scale guides laser treatment selection. Darker skin types have more melanin in the epidermis that competes with target chromophores and is at risk for post-inflammatory hyperpigmentation (PIH) or hypopigmentation:
- Types I–II (fair skin): Full range available including full-field CO₂ and deep chemical peels
- Types III–IV (olive, Asian skin): Prefer fractional techniques (ablative and non-ablative), Er:YAG, medium TCA peels; pre-treat with hydroquinone; avoid high fluences
- Types V–VI (dark brown, Black skin): Non-ablative fractional lasers, long-pulsed Nd:YAG, Q-switched/picosecond lasers with lower fluences; avoid IPL, full-field CO₂, and superficial wavelengths; aggressive pre-treatment and post-treatment hyperpigmentation protocols essential
Combining Lasers with Surgery
Laser resurfacing is frequently combined with surgical procedures performed at the same operative session:
- CO₂ laser + upper blepharoplasty: Resurfacing the lower eyelid and periorbital skin simultaneously with upper blepharoplasty maximizes the rejuvenation result in one recovery period. Full-field lower lid resurfacing should be performed cautiously — cicatricial ectropion is a risk if too much skin is treated near the lid margin.
- Fractionated laser + facelift or brow lift: Skin resurfacing addresses textural changes and fine lines that lifting alone cannot correct.
- Staged treatment: Many physicians prefer to stage laser resurfacing 3–6 months after surgery once swelling has resolved and the surgeon can accurately assess residual skin quality.
Frequently Asked Questions
- What is the difference between ablative and non-ablative laser resurfacing?
- Ablative lasers (CO₂, Er:YAG) remove the outer layers of skin entirely, producing significant collagen remodeling and wrinkle reduction but requiring 7–14 days of healing. Non-ablative lasers heat the dermis without removing the surface — less downtime but subtler results. Fractional lasers (fractional CO₂, Fraxel) treat a fraction of skin at a time, balancing efficacy and recovery.
- Can lasers be used safely around the eyes?
- Yes, with proper technique and eye protection. Oculoplastic surgeons are uniquely trained to treat periorbital skin — the thinnest on the body — with precision. Metal corneal shields are used to protect the eye from laser energy. The periorbital area often shows the most dramatic improvement from resurfacing.
- What is IPL (intense pulsed light) treatment?
- IPL is a broadband light treatment (not a laser) used for vascular lesions (rosacea, telangiectasias), pigmentation, and meibomian gland dysfunction (MGD). For blepharitis and dry eye caused by MGD, IPL applied to the lower eyelid and cheek reduces inflammatory mediators and improves meibomian gland function.
- What should I expect during my laser consultation?
- During your consultation, your oculoplastic surgeon will evaluate your skin type, concerns, and medical history to determine which laser treatment is best suited for you. They will explain the specific procedure, discuss realistic outcomes based on your skin condition, and review before-and-after photos of similar cases. The surgeon will also discuss potential risks, recovery time, and answer any questions you have about the treatment plan.
- What is the typical recovery process after laser skin resurfacing?
- Recovery depends on the type of laser used, but most patients experience redness, swelling, and mild discomfort for several days to weeks. Your surgeon will provide detailed post-operative instructions, which typically include keeping the treated area clean, using prescribed healing ointments, avoiding sun exposure, and limiting strenuous activities. Most patients can return to light daily activities within 1-2 weeks, though complete healing and final results may take several months.
- Am I a good candidate for laser skin resurfacing?
- Good candidates for laser resurfacing are generally in good overall health, have realistic expectations, and want to address specific concerns like fine lines, sun damage, age spots, or rosacea. Certain skin types and conditions may require different laser approaches or extra precautions. Your oculoplastic surgeon will assess factors such as skin tone, thickness, and medical history to determine if you're suitable for treatment and which laser type would work best for you.
- How long do the results from laser treatments last?
- Results from laser skin resurfacing can be long-lasting, especially for ablative treatments, as they stimulate collagen remodeling and produce significant improvement in skin texture and appearance. However, the periorbital area continues to age naturally, and results typically last several years before gradual changes occur. Sun protection and a good skincare routine are essential to maintain results, and some patients choose periodic maintenance treatments to extend the benefits.
Find a Specialist
Connect with a board-certified oculoplastic surgeon who specializes in lasers.
Search the Directory →